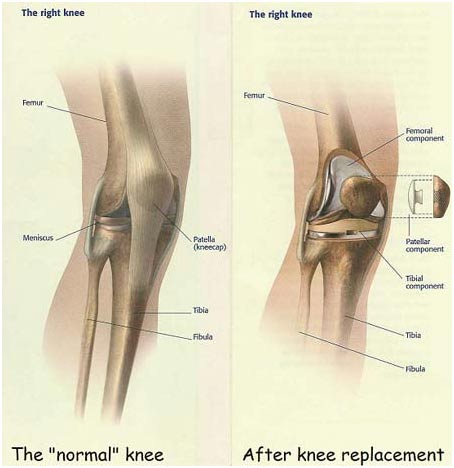
Total knee arthroplasty, sometimes known as total knee replacement, involves the cutting and resurfacing of bone from the end of the femur (thigh bone) and replacement with a metal implant. The top of the tibia (shin bone) is also cut and resurfaced and then replaced with a metal and plastic component. The kneecap (patella) is also resurfaced.
As with any surgery, there are risks inherent with this procedure. The major risks for this procedure are the risks associated with anesthesia, infection, nerve damage, fracture, and blood clots in the legs and lungs. With Dr Mullens minimally invasive technique there is minimal blood loss, there is no need to pre-donate any blood, and only very rarely does a patient require a transfusion.
What do I need for surgery?
Some patients will be sent for blood work and an EKG before surgery. If a heart condition needed to be addressed within the prior year, a letter from your cardiologist describing your condition should be faxed to Dr Mullen.
MEDICATION: Dr Mullen wants you to get TWO (2) medications that you will use AFTER surgery. The first is Aspirin 325 mg taken twice daily to thin your blood after surgery. The second is a prescription pain pill that will be electronically submitted to your pharmacy. Let Dr Mullen know at the pre-operative appointment if you have a preference for any particular pain medicine that works best for you, as it is not safe to send in prescriptions for more than one narcotic. You can pick up both of these before surgery, but they are not to be taken until after surgery is completed.
WALKER: You will need to get a walker and bring it with you to the hospital for surgery. It needs to be the kind with TWO (2) wheels in the front and NO wheels in the back. Walkers with four wheels and hand brakes are dangerous and less appropriate for use immediately after surgery.
CLASS: The hospital may notify you about completing a Pre-Surgical Joint Replacement Class. If notified that the class is required for you, failure to complete this class in a timely manner may result in cancellation of your surgery.
What medicines should I stop taking before surgery?
Plavix (Clopidogrel), Effient (Prasugrel), Pletal (Cilostazol) and NSAIDs (Advil, Aleve, Aspirin, Diclofenac, Ibuprofen, Motrin) need to be discontinued 10 days prior to surgery.
Over-the-counter vitamins often have ingredients that may thin the blood and must be discontinued 7 days prior to surgery.
Coumadin (Warfarin) and Brilinta (Ticagrelor) need to be discontinued 5 days prior to surgery.
Eliquis (Apixaban), Xarelto (Rivaroxaban) and Pradaxa (Dabigatran) need to be discontinued 4 days prior to surgery.
Failure to stop taking these blood thinning agents at these recommended times puts you at significant risk for excessive and potentially life-threatening bleeding, and may result in cancellation of your surgery. If you have any specific concerns with regards to your blood thinners, please address them with Dr Mullen and his office team no later than at your pre-operative appointment.
What kind of Ice Packs should I get?
While at your pharmacy before surgery you may consider obtaining two cold therapy packs that can mold to your knee to use after surgery. Two are nice to have so one can be in the freezer while the other is on your knee. Some people like one on the front and one on the back of the knee at the same time. There are many brands and sizes, most are inexpensive and very helpful with swelling and minimize pain. Alternatively, Polar Care Cryotherapy Units are not covered by most insurance plans but can be found and purchased on Amazon if you prefer. Regular ice packs work well too. Frozen peas are gross and disgusting.
Where will surgery take place?
Dr Mullen has operating privileges at multiple hospitals, but for many reasons he prefers to do most of his knee replacement surgeries at OASIS Hospital on 40th St and North Loop 202. However, some patients with a Banner Insurance Medicare Replacement Plans will be scheduled at Banner Baywood.
All of his patients get a private room.
OASIS Hospital is an orthopedic specialty hospital, and does not admit sick patients, making it a very clean and safer hospital environment.
All of Dr Mullens patients are cared for by a certified orthopedic nurse who will not concurrently have responsibilities for any patients with concomitant infections or contagions. This is very important to Dr Mullen and should be to you. Within this system, there are very few resultant infections.
The physical therapy program targets and often allows for patients to be discharged the very next day. In some cases patients can go home that very same day. Very rarely does a patient need to stay a second night. Planning for a Rehab Center or a Skilled Nursing Facility will not be necessary with his program.
What do I do the night before surgery?
Drink plenty of liquids. Stock your home with easy to prepare meals for a few days.
In order to reduce the chance of infection, we ask you to perform a pre-operative skin prep. Please shower and scrub every day the week preceding surgery and make sure you shower the morning of surgery with regular soap.
You may take your pre-approved medicines the morning of surgery with a sip of water, but may NOT eat or drink anything else the day of surgery. No mints, no gum, no tic tacs nothing.
When do I need to get to the hospital?
You will report to the hospital at least 2 hours before the surgery is scheduled to start. That time is needed for administrative check in, escort to the preop area, changing into a hospital gown, have a nursing evaluation, get an IV, and get a preoperative IV antibiotic infusion through that IV. You will meet your anesthesiologist to both answer and ask questions. Anti-nausea medication can be delivered before surgery through the IV.
What kind of anesthesia will I get?
A spinal anesthesia is typically the safest. This allows for better postop pain control as well as less nausea and a lower complication rate than a general anesthetic. If a spinal anesthetic is contraindicated for some reason, the anesthesiologist will discuss your options with you to make an informed and consensual plan. Regardless of the type of anesthesia, you will not be alert during nor remember the surgery
Adjunctively, your anesthesiologist will give you an Adductor Canal Nerve Block immediately after surgery. This block will numb the nerve in your upper thigh that supplies sensation to a large part of your knee. This minimizes pain, wears off within 12-20 hours, but may leave your leg feeling heavy until it wears off.
How long does the surgery take?
You will arrive at the facility 2 to 3 hours before the surgical start. Once family and friends are eventually shown to the waiting area, you will get some intravenous sedation, be transported to the operating room table and then be safely anesthetized and put to sleep. You will then be comfortably positioned for your surgery, your skin sterilized, and sterile drapes applied. This all takes under an hour. Dr Mullen institutes a series of safety checks and then will perform your surgery. The actual surgery takes about another hour. You then will spend about 90 minutes in the Recovery Room. Your guests will visit with you only after you leave the Recovery Room and are brought to your private room.
How will my pain be controlled?
Your anesthesiologist will give you medicines while you are in surgery to keep you comfortable. So will the nurse in the Recovery Room. The spinal anesthetic and the nerve block last many hours. Once in your room oral pain pills will be available to you every few hours as needed.
Let Dr Mullen know at the pre-operative appointment if you have a preference for any particular pain medicine that works best for you. ALL narcotic pain medicine can result in nausea. This is an undesired adverse side effect, but is not an allergy. This can ideally be combatted by finding and using a narcotic that sits well in your particular stomach. If you are someone who gets nauseated with many different narcotic pain meds, we can use and anti-nausea medicine with your pain pill or just use over the counter pain analgesics like Tylenol instead. This may be a wise strategy if the nausea of a pain pill is more distasteful than the pain itself.
Do I walk on my leg right away?
Yes. The day of surgery. After getting settled in your room you will get out of your bed and walk in your room with supervision using your walker. Depending on the time of day and how you feel, you may go for a walk in the hallway the day of surgery. Dr. Mullen will also have you scheduled for PT the day after surgery. Your goal will be to walk 100 feet down the hallway with your walker before going home.
When will I go home?
Some patients may be allowed to go home the same day as surgery. This is a discharge plan reserved for patients with confidence, a strong upper body, and demonstrable proficiency with their walker. If you are interested in potentially going home the same day as surgery, let your anesthesiologist know and he/she may use a shorter acting spinal so you can walk sooner. However, most patients will stay one night and go home the next day. Rarely is it necessary to stay longer than that. It is even more rare to need to go to a Rehab Center or a Skilled Nursing Center instead of to your home. Remember, you are not sick. When you are mobile enough to get in and out of bed, up from and back into a chair, and up and down the hall, you will go home.
Wouldn’t it be safer to stay longer or go into Rehab?
Not necessarily. Studies have shown an increase rate of infections and medical complications in patients who stayed in the hospital longer or went to a Rehab center before going home. The best plan is to go home.
Where will I do my Physical Therapy?
A team is assembled to help you. Depending on your insurance, Dr Mullen can arrange for a physical therapist to work with you at home 3x/week for two weeks after you get home. Some insurance plans do not allow for this option. Patients with these types of health plans will need to make arrangements for and subsequently begin Outpatient PT the day after discharge.
After the Home Health PT, you then will begin Outpatient PT 2-3 times per week for 6 weeks. Dr Mullen knows many clinics and therapists and can help you choose a PT clinic that does good work, is near your home, and takes your insurance.
Do I get a "Motion Machine"?
CPM or Continuous Passive Motion machines are no longer used in the hospital for the first few days after surgery. This is partially to allow you to rest. Once you go home however, and depending on your insurance again, a CPM machine can be delivered to your home to use for as many as 18 days. It can be used multiple times per day for a total 6 hours of use per day. Although using a CPM machine may help you get your motion back quicker, studies also show that your eventual final range of motion will likely not be influenced greatly by the use of a CPM. You just may get it back quicker. If you find the CPM use uncomfortable, it can be returned to the vendor earlier as it is not mandatory. Most patients find it helpful.
How do I keep from getting a DVT, or a ‘blood clot’?
Many things can help, but DVTs do occur sometimes. Early full weight bearing and frequent walking is the most important and effective way to prevent DVTs. You will be started on Aspirin twice daily to chemically thin your blood right after surgery.
If you already take a prescription daily blood thinner as part of your typical medical regimen, aspirin may not be needed as these prescription blood thinners can be restarted 24 hours after surgery. Ask Dr Mullen and his office team at the pre-operative appointment if you have any questions regarding your blood thinners.
When may I shower and change my bandage?
Dr Mullen will apply an antimicrobial foam adhesive bandage to your knee after surgery that stays on for 7 days. An ACE wrap on top of this adhesive bandage may be removed the day after surgery. The adhesive bandage is water resistant, and you may shower with the adhesive bandage on, dabbing it dry afterwards. However, under no circumstances should the knee be dunked or submerged under water for 6 whole weeks.
7 days after surgery you will peel off the adhesive bandage. You will then see your wound. You may still shower and now get the incision wet, but only let soapy water run along the incision briefly before patting it dry. Keeping your incision clean this way is a good idea and can help prevent infection. Your shower should be brief. Dont linger. After showering you should cover the wound with a piece of gauze and an ACE wrap.
Do not apply any ointments or creams to your incision. You are still not allowed to dunk or submerge your incision under water for 6 weeks. Water exposure in this manner can seep into the incision and cause a terrible infection. That means no bathtubs, hot tubs, Jacuzzis, swimming pools, or water therapy for 6 weeks.
When may I drive?
It is illegal to drive under the influence of narcotics. Once you do not need narcotics, and only after you feel physically able to accept the responsibilities that come with driving a car may you return to driving. That turns out to be an answer that changes patient to patient.
When will I be seen after surgery?
Your next appointment in the office is usually scheduled for about 15 days after surgery.
How long will I be out of work?
Your return to work is dependent on the type of occupation you have. Patients with sedentary jobs may be able to return to work by 4 weeks after surgery. Patients with a physically demanding occupation may be able to return 8-10 weeks after surgery.
Do I need to take antibiotics before dental cleanings forever now?
Conflicting evidence exists regarding their necessity; however, most doctors agree that anyone with any medical condition that increases any risk of infection should use pre-dental care antibiotics. Dental infections or bad teeth can be a source of infection for a total knee even after the surgery is completed. For this reason it is wise to advise your dentist that you have had a total knee replacement surgery. For any dental procedures, including cleaning of your teeth, you should consider antibiotic prophylaxis. This is generally a single oral dose of either Amoxicillin 2 grams or Cleocin 600 mg one hour before dental procedures. Other infections in the body, such as boils or bacterial infection, could also represent a source of problems for a person with total knee replacement. For this reason, if you have any infection you should consult your family doctor promptly so that proper treatment can be carried out.
Are my expectations realistic?
Total knee replacement surgery is major surgery and should not be undertaken lightly. It is wise to keep in mind when considering this surgery that even the best total knee replacement is not as good as your knee was when it was healthy. The goal of the surgery is to relieve your pain, if not totally, then at least somewhat. It is also the goal with this surgery that you will maintain reasonable stability and flexibility as well.
Even when you feel much better you must keep in mind that this new knee is a mechanical device. Just like any mechanical device, including your automobile, there can be problems or failures. In general, total knee replacements can last many years. As with any medical procedure, there is no guarantee.
Even if you feel much better following your surgery it is wise that you avoid activities which require high impact to the knee or hard contusions to the knee. While permitted, they may shorten the lifespan of the knee.