The rotator cuff is made up of four muscles that surround the humeral head (ball). These muscles are attached to the bone by tendons that blend together to form a cuff that surrounds the ball. When the rotator cuff muscles contract, their combined action centers the ball in the deepest portion of the shoulder socket. This centering effect is essential for normal shoulder function and allows the arm to be positioned in an incredibly wide range of motion with both strength and stability.
With increasing age the rotator cuff is prone to tear. Tears can occur from an acute injury, from accumulated damage over time and from tendon weakening that occurs from the aging process. If tears go untreated, they may progress and enlarge over time to involve a substantial portion of the rotator cuff. When two or more tendons are involved, cuff tears are considered massive. Such tears have a major impact on both shoulder strength and stability. Strength is impaired because the muscle is no longer attached to the bone. Stability impaired because the cuff can no longer center the ball in the socket. As a result, the humeral head drifts upward in the socket until it abuts against the acromion bone. Over time, this abnormal relationship between the ball and socket leads to erosion of the upper lip of the socket and arthritis ensues.
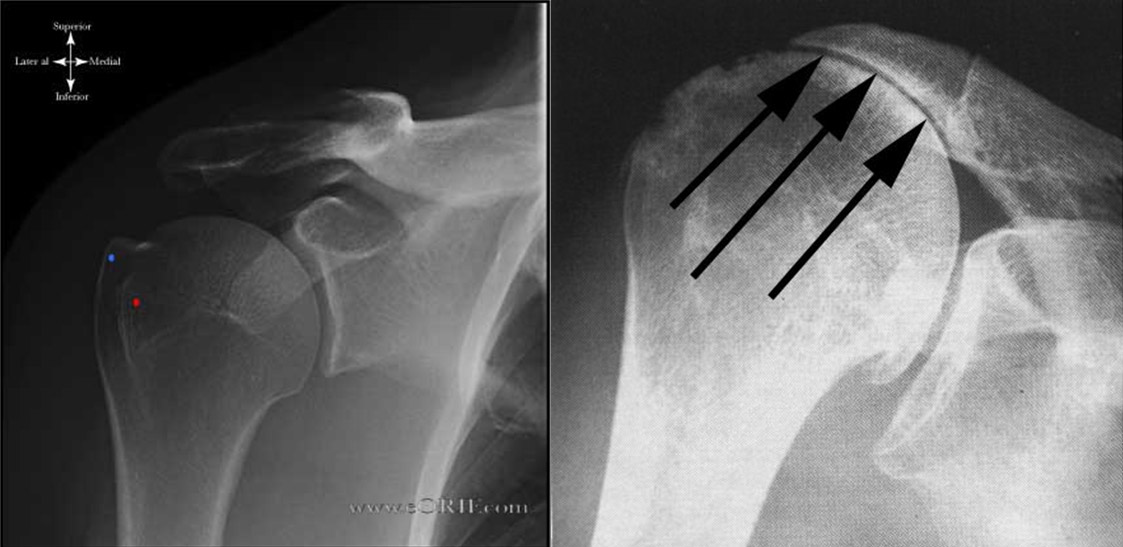
The X-ray to the left shows a normal shoulder. The X-ray to the right shows a shoulder with cuff tear arthropathy. The ball has risen upward causing erosion of the upper socket and abrasion against the acromion bone. The humeral ball has been rounded off from this abrasion.
Other changes occur around the shoulder joint that complicate the management of this condition. First, as a result of a long-standing tear, the rotator cuff muscles atrophy and are replaced by fat. Second, torn tendons undergo further degeneration and thinning both from disuse and abrasion. Third, the bone of the humeral head weakens from disuse. These changes generally make it impossible to repair the rotator cuff, classifying such tears as irreparable. With time, the bone of the humeral head may become so weak that collapse of the head occurs and the ball loses its smooth round joint surface.
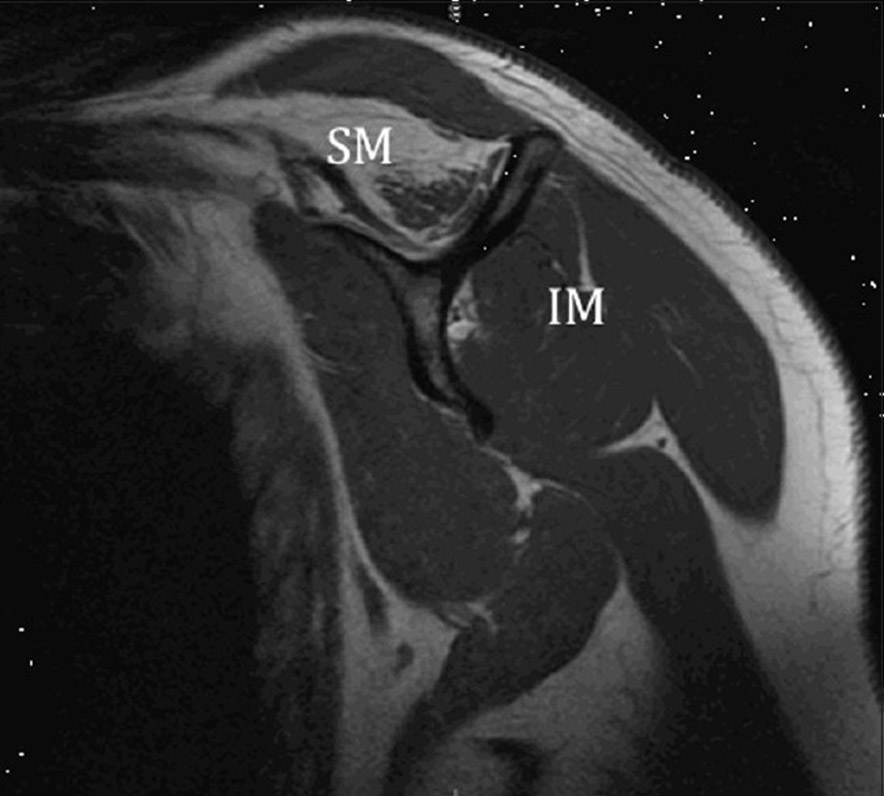
This MRI image shows fatty replacement of the Supraspinatus (SM) muscle but not the Infraspinatus (IM) muscle. The Subscapularis muscle on the left is also normal. Fat appears as white signal on this MRI while muscle appears as dark gray. In the Supraspinatus muscle (SM), notice the muscle appears as just a fraction of this space while fat has replaced a majority of the volume. This fatty replacement is not reversible and muscle bulk and strength cannot be recovered once such atrophy has occurred.
Causes/Risk Factors
Not all massive rotator cuff tears result in cuff tear arthropathy. Some people with massive tears maintain well-compensated shoulder function despite the absence of an intact rotator cuff. The factors that cause certain patients to develop arthritis are not fully understood but it most likely represents a combination of abnormal joint mechanics from upward migration of the ball and loss of joint nutrition from leakage of joint fluid away from the cartilage. Currently we cannot predict which tears will progress to cuff tear arthropathy, nor have we identified any specific risk factors for its development. A more general risk factor is age. As we age, our tendons lose strength because their internal ability to heal and regenerate decreases. Damage that accumulates from repetitive use therefore is more likely to result in a tear compared to younger patients whose tendons are stronger.
Symptoms and Signs
Symptoms:
Severe pain and poor shoulder function are the hallmarks of this condition. Pain is generally aggravated by use but as the arthritis worsens, many patients will develop pain at rest as well. Night pain is also a typical feature and patients may awaken several times from pain. Shoulder function is affected both by pain but also by mechanical failure of the joint. With any attempt to raise the arm, the humeral head migrates upward out of the center of the socket. Without a stable platform for movement, the remaining shoulder muscles are unable to elevate the arm. Thus, many patients develop pseudo‑paralysis due to almost complete inability to lift the arm away from the side. Inward and outward rotation may also be severely restricted depending on the specific tendons torn.
Signs:
Cuff tear arthropathy is generally easy to identify by physical examination. Muscle atrophy results in characteristic wasting about the posterior shoulder girdle. Rotation of the joint causes pain and grinding of the ball against both the socket and acromion. Active elevation of the arm results in a classic shoulder hike as patients try to use the trapezius muscle to lift the arm away from the body by shrugging the shoulder blade. Finally, many patients will have a rupture of the biceps tendon. While these are the typical features of a massive rotator cuff tear, every patient may be affected differently. Despite a massive tear, some patients are able to actively elevate the arm by recruiting the deltoid and other muscles about the shoulder girdle.
How is Cuff Tear Arthropathy Diagnosed?
In some cases, the patient’s history and physical exam may be all that is necessary to make a diagnosis of a cuff tear arthropathy. Nevertheless, imaging studies are important to assess the degree of arthritis, and bony relationships.
Plain X‑rays are essential to confirm the diagnosis. When these show upward migration of the ball in the socket, a massive, irreparable rotator cuff tear is present. These x‑rays also show the degree to which the ball has worn against the upper part of the socket and the undersurface of the acromion. In addition, they show if the ball has undergone any collapse from severe osteoporosis.
If the X‑rays suggest that significant wear has occurred against the acromion undersurface, a CT scan may be necessary to look for the presence of an acromion stress fracture. A CT scan is a special study that takes multiple x‑rays in 3 dimensions and provides greater detail of the bone structure. CT scans also provide more detailed information about the relationship of the ball to the socket and about the pattern of socket wear and erosion.
MRI scans are even more helpful in diagnosing cases of true cuff tear arthropathy. MRIs are useful in looking at the rotator cuff tendons, the size of a tear, the level of retraction of the torn end, the level of muscular atrophy and the amount of fatty infiltration.
What is the Natural History of Cuff Tear Arthropathy?
There is currently no way to predict if and when patients with a massive, irreparable rotator cuff tear will develop arthritis. When this degenerative process occurs, progressive wear and erosion of the socket and acromion occur and osteoporosis of the humeral head may ultimately result in collapse and severe deformity. Most patients seek treatment before collapse occurs. While some patients reach a plateau in terms of pain and loss of function, some patients continue to decline with progressive disability.
These include:
Physical demands
Amount of functional disability
Ability to tolerate and comply with the necessary rehabilitation
Presence of other medical problems that might complicate the effectiveness of surgical treatment
Each case must be individually assessed in terms of these factors to define a treatment regimen that best restores quality of life while minimizing risk to the patient.