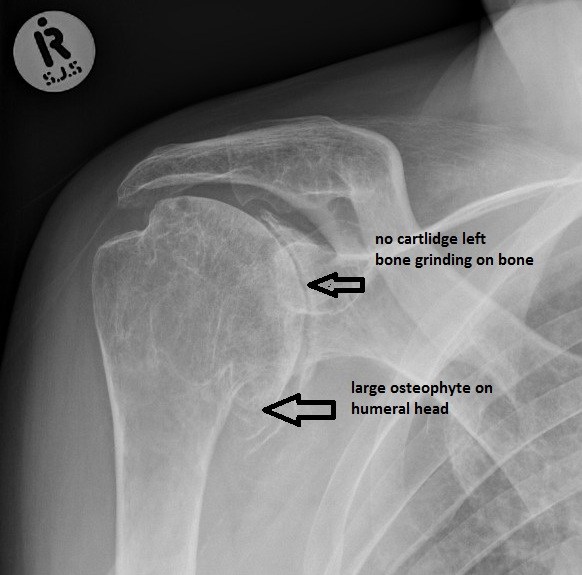
Arthritis of the shoulder is a condition in which the cartilage on the humeral head and glenoid deteriorates. Progressive wearing out of the joint surfaces may expose areas of raw bone. As this process becomes more advanced, the joint surfaces become rough, and joint motion causes friction and abrasion. The capsule surrounding the shoulder joint may become inflamed and contracted. These processes result in pain, stiffness and loss of function. This figure shows the surface of a humeral head destroyed by arthritis. The cartilage has completely worn away in the central area of the ball. The X-rays of a typical arthritic shoulder show complete loss of the joint space with bone-on-bone articulation.
When symptoms begin to interfere with activities of daily of living and negatively impact one’s quality of life, joint replacement surgery may be considered. This is the most reliable solution for shoulder arthritis that has failed to respond to a program of rest, flexibility and strengthening exercises, and anti‑inflammatory medications.
The following sections will describe in greater detail the surgical procedure, the recovery period and the expected long term outcomes after total shoulder replacement surgery. We will also discuss the potential risks and complications, and long term restrictions. Shoulder replacement surgery can improve the mechanics of the shoulder, but cannot make the joint as good as it was before the onset of arthritis. In many cases, the tendons and muscles around the shoulder have been weakened from prolonged disuse before the operation. It can often take months of gentle exercises before the shoulder achieves maximum improvement.
The effectiveness of the procedure depends on the health and motivation of the patient, the condition of the shoulder, and the expertise of the surgeon. Strict adherence to the rehabilitation program maximizes the chances of a good result from shoulder replacement surgery. Maintaining general health, fitness and nutrition as well as abstinence from cigarette smoking all improve the chances of success. The greatest improvements are in the ability of the patient to sleep, to perform activities of daily living, and to perform non‑contact recreational activities.
Considering Surgery
When the normally smooth surfaces of the shoulder joint are severely damaged by arthritis or injury, conventional total shoulder replacement surgery is the most effective method for restoring comfort and function to the joint. There are other surgical options for treatment of arthritis of the shoulder, but none have proven as effective in terms of pain relief and patient satisfaction as shoulder replacement. Arthroscopy or "clean up" operations may be beneficial early in the course of the disease but have not been shown to provide lasting pain relief over the long term. Shoulder fusion operations prevent any motion at the ball and socket joint. While this is effective in terms of pain relief, patients are limited in terms of mobility and function. Removing the joint, or resection arthroplasty, allows some motion at the joint, but does not provide for strength and return to functional activities.
Who should consider shoulder replacement?
Shoulder replacement surgery is considered when:
The shoulder arthritis is a major problem that negatively impacts one’s quality of life,
One is sufficiently healthy to undergo the procedure,
One understands and accepts the risks and alternatives,
There is sufficient bone and tendon to permit the surgery, and
The surgeon is experienced in the technique of shoulder replacement
What happens without surgery?
The natural history of arthritis is that it usually continues to progress over time. The rate of progression varies between individuals and is unpredictable. Sometimes the pain and stiffness from shoulder arthritis will stabilize at a level that is acceptable and manageable to the patient. In general, this surgery is elective, and can be performed whenever the patient decides that the arthritis has become disabling enough to warrant treatment. In the case of osteoarthritis delaying surgery typically does not compromise the success of surgery in the future.
Long‑term considerations
As with joint replacement procedures in other parts of the body, the components used in the replacement do not last forever. Much like the brakes of a car wear out with use, the plastic socket used in total shoulder replacement surgery also tends to wear with time. It stands to reason that younger patients are more likely to experience socket wear in the course of their life as the plastic is exposed to a longer period of use. In addition, patients who remain physically active often place higher demands on the shoulder. As more people continue to engage in sports and other demanding recreational activities into their 60s, 70s and 80s, shoulder replacements are being asked to tolerate more wear and tear often the same level of use that may have predisposed the shoulder to develop arthritis in the first place. In certain cases of very active patients, loosening of the shoulder socket can occur after surgery. Recognizing this potential risk, younger and more physically active patients sometimes may be better off with a partial joint replacement that does not resurface the arthritic socket.
Effectiveness
Shoulder replacement surgery for osteoarthritis has proven an effective means of restoring lost comfort and function to the shoulder. One must recognize, however, that certain limitations in mobility and strength may persist following surgery. This is because the muscles, tendons and ligaments around the shoulder joint may be contracted or atrophied from the arthritis process. Some of these changes may not be reversible with surgery.
There are several factors that influence the effectiveness of surgery and must be considered in light of the decision to undergo shoulder replacement:
Surgeon experience: It is well documented in the medical literature that surgeons and hospitals that perform more shoulder replacement procedures have a lower complication rate and better long‑term outcomes. Dr. Mullen performs as many shoulder replacements as nearly any doctor in the state.
Patient expectations: If patients have unrealistic expectations about activities or vocations to which they can return following shoulder replacement, they will likely be dissatisfied with the process. If one is unwilling to give up activities that may jeopardize the function of the artificial components, replacement surgery should not be considered.
Compliance with the rehabilitation: A good operation is only half the battle. Participation in a structured rehabilitation and adherence to a home exercise program are essential to recovery of motion, strength and function. Shoulders do not recover on their own, and patients must take a responsible and active role in the process. Thus, the patient’s motivation and dedication are important elements of the partnership.
In general, 90% of patients report good to excellent outcomes following shoulder replacement surgery.
Urgency
Shoulder replacement surgery for osteoarthritis is an elective procedure that can be scheduled when circumstances are optimal for the patient. It is not an urgent procedure. The patient has plenty of time to become informed about the process of surgery and recovery.
Factors that the patient should consider in choosing the optimal time include the following:
The arthritis has become sufficiently disabling to impair the performance of daily activities. Patients who are still able to sleep comfortably and manage daily activities may and probably should consider waiting;
A planned period of time can be dedicated to the recovery and rehabilitation process that will not interfere with other scheduled events;
Overall health and nutritional status are optimal and will not limit the ability to comply with the performance of rehabilitation;
Motivation and readiness to undertake the process of surgery, recovery and rehabilitation is a priority.
Preparing for Surgery
The success of surgery depends on a partnership between the patient and the experienced shoulder surgeon. Patients should optimize their health so that they will be in the best possible condition for this procedure. Smoking should be stopped a month before surgery and not resumed for at least three months afterwards to maximize the body’s healing potential. Any heart, lung, kidney, bladder, tooth, or gum problems should be managed before surgery. Any infection may be a reason to delay the operation. Dr. Mullen needs to be aware of all health issues, including allergies and the nonprescription and prescription medications being taken. Some of these may need to be modified or stopped. For instance, aspirin and anti‑inflammatory medication may affect the way the blood clots. If patients take blood‑thinning medications such as Coumadin, they should check with their primary care physician about the safety of stopping their use 5‑7 days prior to the procedure. These medications can usually be resumed the day following surgery.
The incision for a shoulder replacement extends across the front of the shoulder from the outside end of the collar bone to the mid‑aspect of the upper arm. This area must be kept clean and free from cuts or scratches leading up to the surgery. Plans for necessary assistance need to be made before surgery. For individuals who live alone or those without readily available help, arrangements for home help during the early recovery period should be made well in advance. Many patients will benefit from a stay in a rehabilitation facility for a period after the surgery until they are sufficiently recovered to manage with daily activities.
The Surgical Team
Shoulder replacement surgery is a technically demanding procedure that should be performed by an experienced surgeon in a medical center accustomed to performing shoulder joint replacements at least several times a month. While most general orthopaedic surgeons perform 1‑2 hip or knee replacements a month, the average surgeon may only perform 1 shoulder replacement per year. Dr. Mullen is extensively trained in these procedures, having performed advanced specialty training in the field of shoulder surgery in one of the busiest shoulder replacement centers in the country. This included training in the management of complex and failed shoulder replacements. He has performed as many total shoulder replacements as nearly any surgeon in the state. Our surgical team includes dedicated staff experienced in performing these procedures and we carefully select our implants based on the best products available for individual cases.
About the surgery
Technical details
Shoulder replacement for osteoarthritis is a highly technical procedure; each step plays a critical role in the outcome.
After the anesthetic has been administered and the shoulder is prepared, an incision is made across the front of the shoulder from the middle of the collarbone to the middle of the arm bone. This incision allows access to the joint without damaging the important deltoid or pectoralis muscles that are responsible for a significant portion of the shoulder’s power.
The muscles and other tissues near the shoulder are mobilized by removing any scar tissue that may restrict their motion. The tendon of the subscapularis muscle is cut to gain access to the joint and released circumferentially to restore its length and mobility. The arthritic humeral head is resected along with the bone spurs that surround it. This cut must be carefully planned and oriented to recreate one’s anatomy with the reconstruction. The humeral implant is chosen by trialing different sizes and selecting the one that best matches the patients anatomy and best restores the muscle balance in the joint without making the joint too tight or too loose.
The arthritic glenoid is then exposed removing all bone spurs from its periphery. Adequate exposure is a challenging process, and the surgeon must be familiar with the location of important nerves and blood vessels. A special reamer is used to refinish the glenoid surface in preparation for the prosthesis. This reaming process corrects the shape and orientation of the socket, both of which are affected by shoulder arthritis. Several small holes are then drilled into the socket and filled with bone cement to accept the pegs of the glenoid prosthesis. The prosthesis is inserted and held in place until the cement dries.
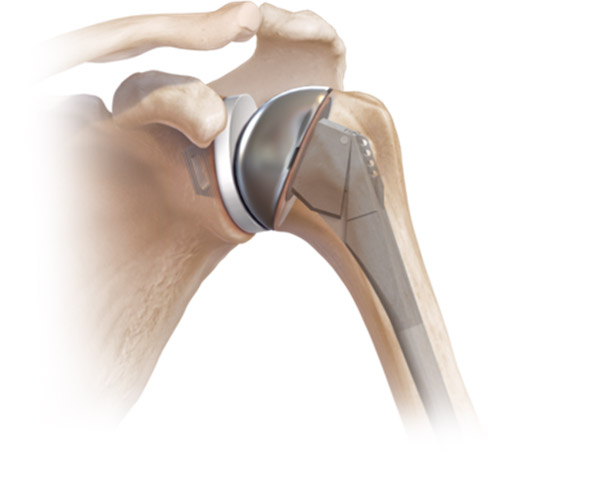
A trial head is placed on the humeral prosthesis to determine proper sizing and muscle balance. The final humeral components are then inserted and the joint is relocated. The subscapularis tendon is then carefully repaired back to the bone and closure of the muscle and skin layers completes the procedure. A drain is placed which is removed on the second morning after surgery. This prevents blood from collecting in the wound. The figure to the right shows a well‑placed prosthesis that restores the anatomical relationship between the ball and socket and recreates a smooth and balanced articulation.
Anesthetics
Shoulder replacement surgery may be performed under a general anesthetic or under a brachial plexus nerve block. A brachial plexus block can provide anesthesia for several hours after the surgery. The patient may wish to discuss their preferences with the anesthesiologist before surgery.
Length of surgery,
The procedure usually takes approximately one and a half hours, however the preoperative preparation and the postoperative recovery may add several hours to this time. Patients often spend two hours in the recovery room and an overnight stay in the hospital after surgery.
Risk and Potential Complications
Complications related to shoulder replacement surgery can be divided into those that occur during surgery, those that occur soon after surgery and those that occur at a time remote from the surgery
Complications during the procedure include:
Injury to the axillary nerve or brachial plexus: These nerves control the muscles of the shoulder and arm. They may be injured by being overstretched during the surgical exposure or by being severed. This is extremely rare and surgeons experienced in shoulder replacement can generally minimize this risk through proper surgical technique
Fracture of the humerus bone: This can occur during insertion of the metal stem. Again, it is rare and can be avoided through careful attention to surgical technique
Complications that occur soon after surgery include:
Wound infection is the main problem that can occur in the early recovery period, generally between 1‑3 weeks. Symptoms include fever, weakness, fatigue and nausea. Signs include redness, swelling and wound drainage. If infection is diagnosed and treated early, it can be managed by an irrigation and debridement operation with preservation of the replacement. If however, the infection is long standing, the artificial components may have to be removed and a staged reconstruction performed after thorough antibiotic treatment.
Rupture of the subscapularis tendon repair may also occur prior to full tendon healing. Overaggressive physical therapy or an accidental fall may cause this. Generally, this necessitates an exploratory surgery along with repair or reconstruction of this tendon.
Stiffness can occur secondary to scar tissue that forms between tissue layers. Generally, with a properly conducted physical therapy program, this is not a problem. However, some patients have an overactive healing response and stiffness may be unavoidable. Stiffness may require a manipulation under anesthesia if further physical therapy cannot improve the range of motion.
Complications that occur remote from surgery:
Socket failure through loosening, wear or fracture is the leading cause of revision surgery. The rate at which this occurs is not known with certainty and may differ depending on the demands placed on the shoulder replacement.
Late infections may occur by spreading to the shoulder from a different source such as the urinary tract, a tooth abscess, or other breaks in the skin. For this reason, we generally recommend that prophylactic antibiotics be taken prior to any invasive procedures such as dental work, colonoscopy, etc.
Recovering from surgery
Pain and pain management
Recovery of comfort and function after shoulder replacement continues for the first year after surgery. Adequate pain control is an important part of the postoperative management because it facilitates rehabilitation and allows recovery of motion. Immediately after surgery, strong medications (such as morphine) are often given by injection. Within a day or so, oral narcotic pain medications are usually sufficient. These oral narcotic medications are generally only needed for a few weeks and patients are encouraged to wean off of them to regular Tylenol when sufficiently comfortable.
Pain medications can be very powerful and effective. Their proper use lies in balancing their pain relieving effect and their other, less desirable effects, such as sedation. Pain medications can cause drowsiness, slowness of breathing, difficulty in emptying the bladder and bowel, nausea, vomiting and allergic reactions. Patients who have taken substantial narcotic medications in the recent past may find that usual doses of pain medication are less effective. For some patients, balancing the benefit and the side effects of pain medication is challenging. Patients should notify their surgeon if they have had previous difficulties with pain medication or pain control.
We generally discourage the use of anti‑inflammatory medications (such as Ibuprofen, Advil, Motrin, Naprosyn, Aleve, and Celebrex) unless patients require their use for other conditions. These medications may slow down the healing of the subscapularis tendon. Ice is used to decrease pain and inflammation during the initial recovery and for several weeks during rehabilitation.
Hospital Stay and Hospital Discharge
Patients generally remain in the hospital overnight following shoulder replacement surgery. Criteria for discharge either to home or to a rehabilitation hospital include:
A clean and dry incision without signs of infection
Normal bowel and bladder function
Adequate pain relief with oral pain medications
Ability to properly perform and comply with home range of motion exercise program
Adequate support to ensure patients are safe
Because the surgical repair must be protected by limited use of the arm during the first 6‑8 weeks after surgery, one must be prepared to manage daily activities with very limited use of the involved arm. Usually the patient is asked to lift nothing heavier than a cup of coffee during this time. Patients usually require some assistance with self‑care, activities of daily living, shopping and driving for approximately six weeks after surgery. Management of these limitations requires advance planning to accomplish the activities of daily living during the period of recovery.
Rehabilitation
Recovery and rehabilitation in the hospital
Early motion after shoulder replacement surgery helps achieve the best possible shoulder function. Arthritic shoulders are stiff. Early motion is facilitated by the complete surgical release of the tight tissues so that after surgery the patient has only to maintain the range of motion achieved at the operation. However, after surgery, scar tissue will tend to recur and limit movement unless motion is started immediately. Early motion also stimulates recovery of muscle function.
During the hospitalization, the patient learns a simple rehabilitation program that will be used for maintaining the range of motion after discharge. This program consists of self‑assisted forward elevation and external rotation, elbow flexion and extension and grip strengthening. Either on the day of surgery, or the day following surgery, the physical therapist will work with the patient to ensure proper technique and understanding of the program. Walking and use of the arm for gentle activities are encouraged soon after surgery.
Outpatient Physical Therapy
Recovery of mobility, strength and function is a graduated process that follows tissue healing. We have developed comprehensive therapy protocols that are designed to prevent recurrent stiffness and re‑educate the muscles about the shoulder girdle to function in a smooth and coordinated fashion. These protocols are designed in such a way for the therapist to educate the patients about home exercises throughout the recovery process. The exercises that a patient does on his/her own between therapy sessions are equally as important as the sessions themselves, and patient adherence to this program is critical to preventing early stiffness. A properly performed home exercise program ensures that the exercises are done frequently, effectively and comfortably.
The early recovery period focuses on maintaining the range of motion achieved by release of scar tissue during the surgery. Strengthening exercises are not performed for the first 6 weeks to prevent stress on the subscapularis repair. A sling is worn between exercise sessions for the first month and then may be discontinued. Patients may use the hand for holding objects like a cup of coffee or newspaper but nothing more than 1‑2 lb. By 6 weeks, gentle active use of the arm for daily activities may be resumed but no heavy lifting, pushing or pulling is allowed. Therapy focuses on a continued flexibility program with aim of a progressive return to full range of motion. Muscle re‑education begins with light resistance exercises for the rotator cuff and the muscles that stabilize the shoulder blade.
By 3 months patients, may resume full use of the extremity provided they have achieved a functional active range of motion. Progressive strengthening exercises with increased resistance and endurance exercises like swimming, rowing, and upper body ergometer are encouraged. In addition, we strongly encourage an aerobic conditioning program for the lower extremities to promote general health and fitness.
By following this exercise program, patients are almost always satisfied with the increases in range of motion, comfort and function that they achieve during the recovery period. If the exercises are uncomfortable, difficult, or painful, the patient should contact the therapist or surgeon promptly.
Maintenance Rehabilitation
Once the range of motion and strength goals are achieved, the exercise program can be cut back to a minimal level. However, gentle stretching is recommended on an ongoing basis. In addition, a maintenance program to keep the rotator cuff muscles strong and healthy will ensure proper function of the artificial joint and may help prolong its benefit.
Return to Functional and Recreational Activities
With the consent of their surgeon, patients can often return to activities such as swimming, golf and tennis at 4‑6 months after their surgery. It is critical that patients achieve sufficient range of motion and strength in advance to prevent muscle fatigue and to undue stress on the artificial components.
Long‑term Patient Limitations
Activities that involve significant impact loading to the shoulder joint (such as chopping wood, contact sports, heavy weight lifting, hammering, etc) may jeopardize the performance of the joint replacement. These types of activities increase the risk for loosening, wear and fracture of the artificial socket and may also risk sprain or tear of the rotator cuff. Thus, patients should take caution in these types of activities to minimize the risk of damage to the operated shoulder.
How long will the shoulder replacement last?
A properly performed shoulder replacement generally lasts 20 years. Factors that determine the longevity of the prosthesis include age, hand dominance, physical demands, and compliance with limitations among others. The duration of comfort and function afforded by a shoulder replacement cannot be predicted in advance in any given case. Revision surgery for a failed shoulder replacement often involves removing a worn or broken socket. These procedures are very technically demanding but generally successful in restoring shoulder function. In general, however, the results of revision shoulder replacement are not as good as for primary shoulder replacement.